The bottle sits on the kitchen counter, still sealed, next to the coffee mug. Your doctor handed you the prescription a week ago, and you have been circling it ever since. A friend swears her statin gave her aches she never had before. A relative says hers has been quietly working for years and she barely notices it. Somewhere in the middle of those two stories is your own body, your own numbers, and a decision that deserves more than a rushed five minutes in a doctor’s office. If that bottle is sitting on your counter too, this is for you.
This is general educational information, not medical advice. Nothing here replaces a real conversation with your own doctor or pharmacist, who knows your history, your medications, and your numbers. Think of what follows as a way to walk into that conversation feeling informed rather than anxious, so you can ask better questions and make a choice that fits your life.
Why Doctors Reach for Statins in the First Place

Cholesterol is not the villain it gets painted as. Your body actually needs it to build cells and make certain hormones. The trouble starts when there is too much of one kind, low-density lipoprotein, often shortened to LDL and nicknamed the “bad” cholesterol. According to the Cleveland Clinic, LDL earns that label because it builds up inside artery walls, narrowing the space blood needs to move through. Over years, that buildup raises the risk of a heart attack or stroke.
Statins work upstream of all that. As Mayo Clinic explains, they block an enzyme the liver uses to make cholesterol, which prompts the liver to pull more cholesterol out of the bloodstream. Some statins can lower LDL by half or more. The common names you may recognize include atorvastatin, rosuvastatin, simvastatin, pravastatin, lovastatin, fluvastatin, and pitavastatin. Lowering LDL is not the whole point, though. The real goal is reducing the chance of the events nobody wants, the heart attack and the stroke. Large bodies of research show that lowering LDL with these medications meaningfully cuts cardiovascular risk, and that benefit shows up in both women and men.
That last point matters more than it sounds. For a long time, heart disease was framed as a man’s problem, which left a lot of women under-screened and under-treated. The truth is that heart disease is a leading cause of death in women, and the protective effect of lowering cholesterol applies to women too. Research summarized in reviews of lipid-lowering therapy notes that while the exact size of the LDL drop can differ somewhat between women and men, the reduction in cardiovascular risk is comparable. A statin is not a men’s medication that women happen to take. It is a tool that works for both.
The Midlife Shift That Changes the Conversation

Here is something that does not get talked about nearly enough at the gynecologist’s office. Cholesterol often changes during the menopause transition. The American Heart Association and Cleveland Clinic both note that as estrogen declines, LDL, triglycerides, and total cholesterol tend to rise, while the protective HDL, the “good” cholesterol, may dip. Before menopause, higher estrogen levels appear to offer women some protection, which is part of why heart disease tends to show up later in women than in men.
What this means in practice is that a woman who has spent decades with reassuringly low cholesterol numbers can be genuinely surprised when, sometime in her forties or fifties, those numbers climb without any obvious change in how she eats or moves. It is not a personal failing. It is biology shifting underneath you. This is also why a statin conversation often lands in exactly this season of life, when a lot is already changing and the last thing you want is one more thing to worry about. Understanding why the number went up can take some of the sting out of the recommendation. Your body is not betraying you. It is doing what bodies do at this stage, and the medication is one response among several.
What Statin-Associated Muscle Symptoms Actually Are
Now to the worry that probably sent you searching in the first place. The muscle aches. Clinicians have a name for this whole category: statin-associated muscle symptoms, sometimes abbreviated SAMS. It covers a wide spectrum, and lumping the whole spectrum together is where a lot of fear comes from.
At the mild and by far most common end, people describe soreness, tenderness, tiredness, or weakness in the muscles. Mayo Clinic notes this can feel like anything from minor discomfort to something annoying enough to interfere with daily activities. It often shows up in larger muscle groups like the thighs, shoulders, or back, and it tends to affect both sides of the body rather than one isolated spot.
At the far, rare end of the spectrum sits a serious condition called rhabdomyolysis, in which muscle tissue breaks down and releases substances that can harm the kidneys. It is the scenario that headlines love and that quietly terrifies people. It is also genuinely rare. Mayo Clinic puts it plainly: only a few cases of rhabdomyolysis occur per million people taking statins, and it tends to happen when statins are combined with certain interacting medications or taken at high doses. The signs of something serious are worth knowing, not to scare you but to give you a clear line: severe muscle pain, dark or cola-colored urine, or extreme weakness are reasons to call your doctor promptly rather than wait. Knowing that line exists is what lets you relax about the everyday twinges that are not it.
The Nocebo Effect, and Why It Is Good News
This next part is one of the most useful and least-known pieces of the whole picture. When researchers run carefully blinded trials, the kind where neither the patient nor the doctor knows who is getting the real statin and who is getting a placebo sugar pill, something striking happens. The rate of muscle symptoms in the statin group often looks remarkably similar to the rate in the placebo group. People taking a pill with no active medication report muscle aches at rates close to those taking the real thing.
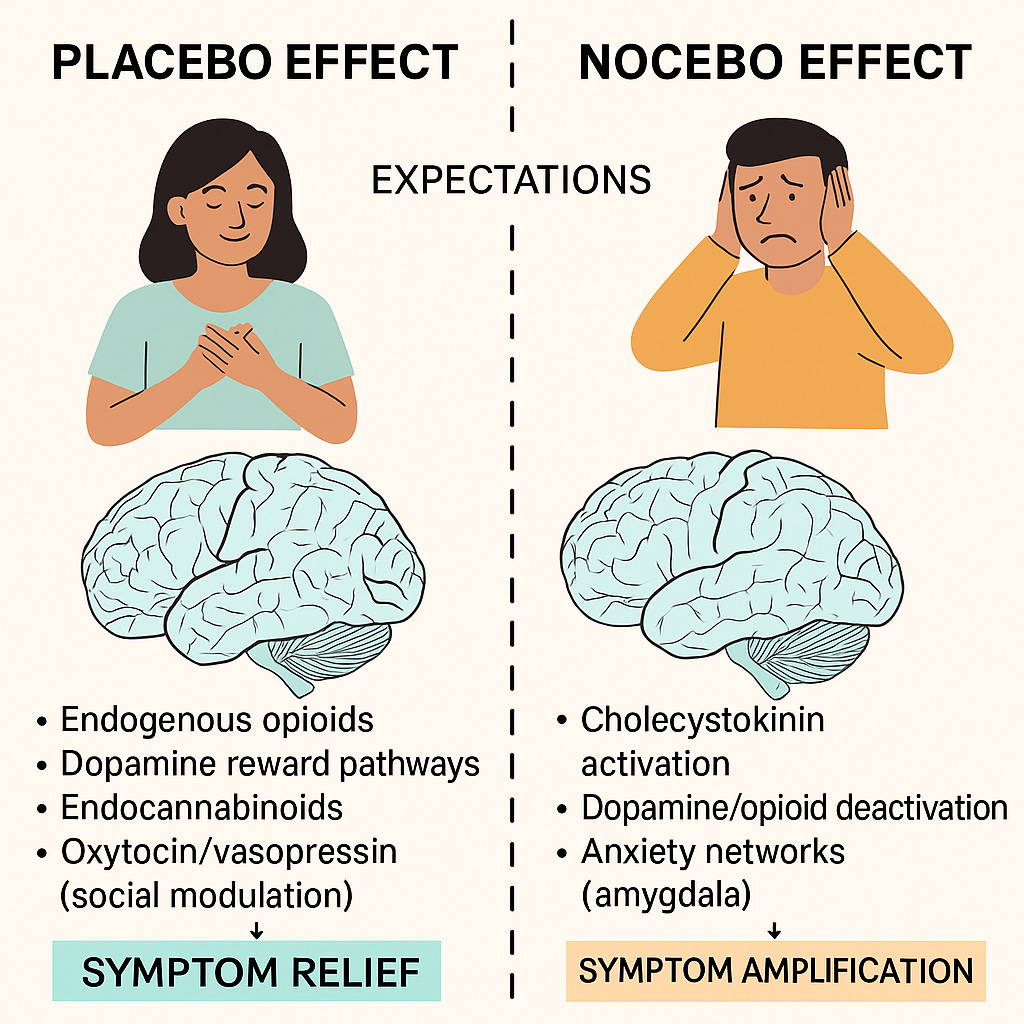
This is the nocebo effect. It is the flip side of the placebo effect. Where a placebo can make people feel better because they expect to, a nocebo can make people feel worse because they expect a side effect. Mayo Clinic states that the real risk of developing muscle pain specifically from a statin is about 5 percent or less compared with a placebo, and that one of the strongest predictors of whether someone reports muscle aches is simply whether they read about that side effect beforehand. Researchers writing in The Lancet and related work have described how a large share of reported statin muscle symptoms may trace back to expectation rather than the drug itself, a phenomenon some have nicknamed the “drucebo” effect.
It would be easy to hear this as “your pain is in your head,” and that is absolutely not the point. Pain is real whether its source is the drug, anxiety, ordinary aging, a tough workout, or some combination. The genuinely empowering takeaway is different and gentler. A lot of the muscle pain people fear when starting a statin is not destiny. If you begin treatment without bracing for misery, you may simply do fine. And if symptoms do appear, the picture is rarely as grim or as fixed as the internet suggests. That knowledge is a quiet form of protection.
Why Women, Especially Over 40, Deserve a Closer Look

Statins are not one-size-fits-all, and a few factors stack up in ways that are worth naming directly for women. Mayo Clinic lists being female and having a smaller body frame among the risk factors that can raise the odds of statin side effects. Other factors on that list include taking the highest dose of a given statin, taking more than one cholesterol-lowering drug at once, being older, having kidney or liver disease, having an underactive thyroid, or drinking heavily.
Several of those intersect with women’s lives in midlife and beyond. Thyroid conditions, for instance, are more common in women, and an underactive thyroid that has not been well managed can itself cause muscle aches and can raise the risk of statin-related muscle symptoms. A smaller body frame can mean a standard dose lands differently. Kidney function naturally shifts with age. None of this means a woman should avoid statins. It means the starting dose, the specific statin chosen, and the other medications already in your cabinet all deserve a thoughtful look rather than an autopilot prescription.
Drug interactions belong at the center of that look. Certain medications raise statin levels in the body and, with them, the chance of muscle trouble. Mayo Clinic names examples including some heart-rhythm drugs, certain antibiotics and antifungals, some HIV treatments, particular immune-suppressing drugs, and another cholesterol medication called gemfibrozil. Even grapefruit and grapefruit juice can interfere with how some statins are broken down, which is why your pharmacist may ask about it. The practical move is simple. Make sure whoever prescribes your statin has a complete, current list of everything you take, including supplements, because that list is one of the biggest levers for keeping you comfortable and safe.
How to Have the Conversation Without Losing Your Nerve
A good appointment is one you have prepared for, and you do not need a medical degree to prepare well. Bring your real questions and your real history, and treat the visit as a two-way decision rather than a verdict handed down to you.
A few questions tend to open up the most useful discussion. You might ask what your actual cardiovascular risk looks like and how much a statin is expected to lower it, so the benefit feels concrete rather than abstract. You can ask which statin and which dose your doctor recommends and why, since some statins are more prone to muscle complaints at higher doses than others. It is fair to ask whether starting low and adjusting makes sense for you, and whether an every-other-day approach is ever appropriate for your situation. Ask what specifically should prompt a call, so you leave with a clear sense of normal versus worrisome. And hand over that full medication and supplement list so interactions can be checked before you ever swallow the first pill.
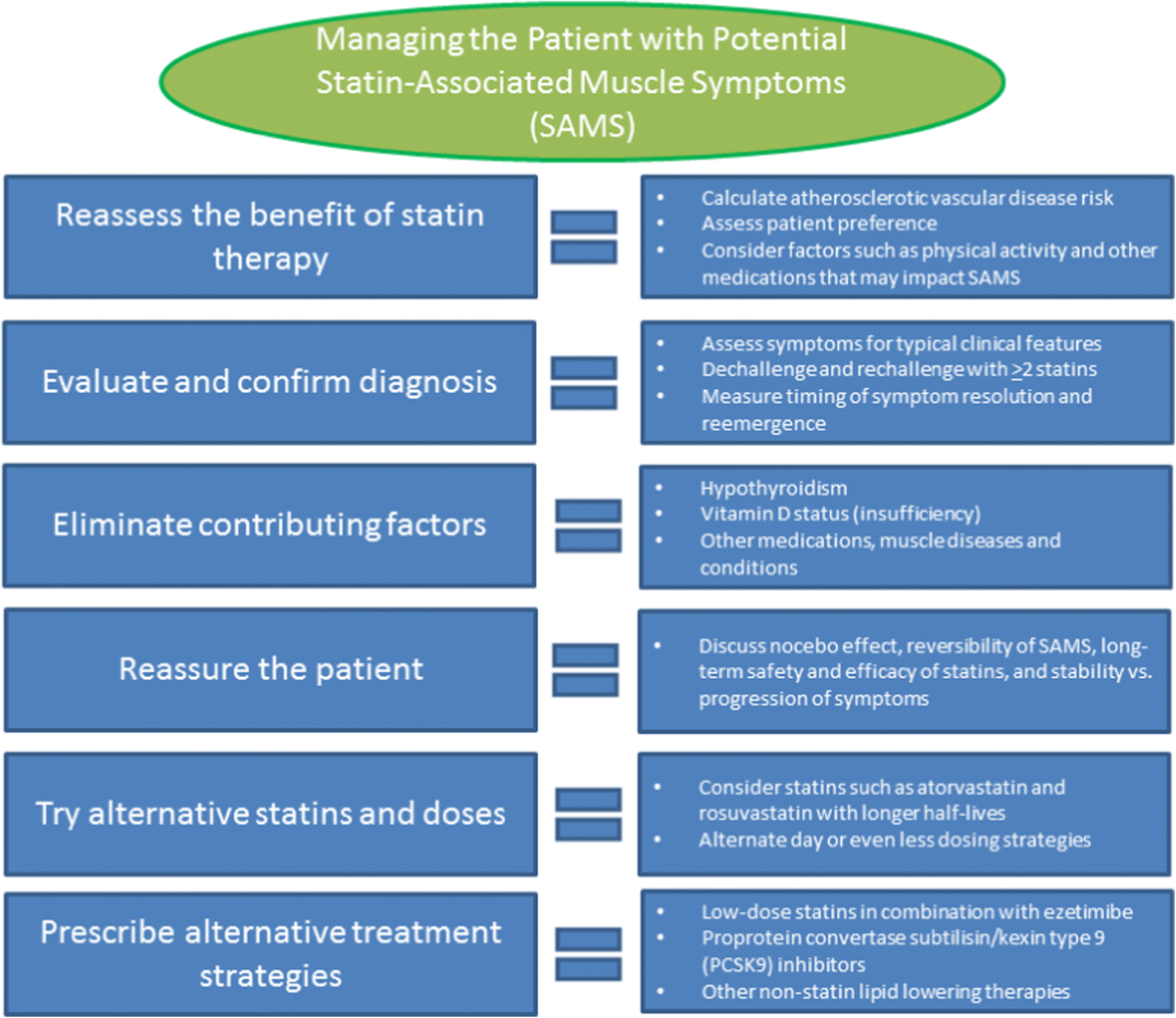
If you start a statin and muscle symptoms do show up, there is a real menu of options, and stopping cold on your own is not the recommended first move. Mayo Clinic describes approaches a clinician might consider, such as a short, supervised pause to see whether the aches truly track with the medication, switching to a different statin, lowering the dose, or pairing a lower statin dose with another cholesterol-lowering medicine. Sometimes the aches turn out to be ordinary midlife stiffness or a new exercise routine rather than the pill at all, and a planned pause is how you find out. The point is that there is almost always a next adjustment to try.
Why Stopping On Your Own Is the One Move to Avoid
If you remember a single sentence from all of this, make it this one. Do not stop a prescribed statin on your own without talking to your doctor or pharmacist first. The reasoning is straightforward and worth sitting with. High cholesterol does not announce itself. It causes no symptoms while it quietly raises your risk of a heart attack or stroke, which means the medication can feel pointless precisely because it is working invisibly. Walking away from it because of an ache trades a manageable, often addressable discomfort for a real and silent cardiovascular risk.
The honest, balanced picture is that statins carry genuine benefits and, for some people, genuine side effects, and the two have to be weighed together rather than one at a time. For most people, the protection against heart attack and stroke outweighs the risks, and serious side effects are very rare. For the smaller number who do struggle with muscle symptoms, the answer is rarely “give up” and almost always “adjust.” Both of those paths run through your doctor, not around them.
So here is where the bottle on the counter goes. Pick it up, and bring it and your questions to someone who can see your whole picture. You are allowed to want both things at once: a heart that is protected for the decades ahead, and a body that feels like yours day to day. Those goals are not in conflict, and you do not have to choose between staying quiet and stopping cold. The middle path, the informed conversation, is the one that keeps both your heart and your comfort on the table. That conversation is yours to start, and you are more ready for it now than you were when that bottle first arrived.