A phone call landed in the Evert family in late 2021 that would change the course of one of tennis’s most decorated careers, though it had nothing to do with a trophy or a comeback. Years after her younger sister Jeanne died of ovarian cancer, the laboratory that had studied Jeanne’s case reclassified a genetic finding. A variant once filed away as uncertain was now understood to be meaningful. That single update, passed from a sister who was gone to a sister who was still here, set in motion a chain of decisions that an 18-time Grand Slam champion has since spent years asking other women to learn from.
This article shares general educational information about ovarian cancer awareness and self-advocacy. It is not medical advice, and it cannot replace a conversation with your own doctor. If you have symptoms, a family history that worries you, or questions about screening, please bring them to a qualified healthcare provider who knows your full history. With that grounding in place, the story of how one of the most disciplined athletes of her generation came to a diagnosis is worth sitting with, because the lessons in it belong to everyone.
A Diagnosis That Started With a Sister’s Story
Chris Evert publicly shared her ovarian cancer diagnosis in January 2022, writing about it in her own words for ESPN. The path to that announcement is the part worth holding onto. Her sister, Jeanne Evert Dubin, herself a former professional tennis player, had been diagnosed with ovarian cancer and died of the disease in February 2020. As Evert has explained publicly, it was genetic information drawn from Jeanne’s case that later pointed the rest of the family toward testing.
Evert underwent genetic testing and learned she carried a pathogenic variant in the BRCA1 gene, a finding linked to a higher risk of ovarian and breast cancers. Acting on that knowledge, she chose to have a preventive hysterectomy in December 2021. She did not have symptoms. She felt well. The surgery was a precaution rooted in what her genes and her family history were telling her. When the pathology came back after surgery, doctors had found malignant cells, and she was diagnosed with stage 1C ovarian cancer, an early stage that is far less common to catch than the advanced disease most women are diagnosed with.
In her own public account, Evert has been direct about what that timing meant. The cancer was found early because she went looking, prompted by her sister’s experience and a genetic result, not because a routine test flagged it. That distinction sits at the center of everything ovarian cancer awareness tries to teach. There was no scan on a calendar that caught this. There was a family story, a willingness to investigate it, and a decision to act.
Why Ovarian Cancer Is So Hard to Catch Early
Ovarian cancer carries a difficult reputation, and the reasons are worth understanding clearly rather than fearfully. The biggest challenge is that there is no reliable routine screening test for ovarian cancer in women at average risk. This is not an oversight or a gap waiting to be filled next year. Major medical bodies, including the American College of Obstetricians and Gynecologists and the U.S. Preventive Services Task Force, currently recommend against routine screening of women who are at average risk and have no symptoms.
That guidance can feel counterintuitive, especially in a culture that treats screening as universally good. The reasoning, as these organizations explain, is that the available tools, such as transvaginal ultrasound and the CA-125 blood test, have not been shown to lower the number of deaths from ovarian cancer when used broadly on women without symptoms or elevated risk. Instead, they tend to produce false alarms that lead to additional testing and surgeries that turn out not to be needed. A test that creates more harm than benefit is not a test worth recommending for everyone, and that honesty matters.
This is precisely why personal awareness carries so much weight with ovarian cancer. The Pap test, a familiar part of many women’s routine care, screens for cervical cancer and does not detect ovarian cancer. That surprises a lot of people. A normal Pap result is reassuring about the cervix, but it says nothing about the ovaries or fallopian tubes. Understanding what your regular care does and does not cover is part of being an informed patient, and it is one of the quiet, practical takeaways inside Evert’s very public story.
The Symptoms Worth Knowing - And the Pattern That Matters

If routine screening is not the answer for most women, paying attention to your own body becomes far more important. The American Cancer Society describes a recognizable cluster of symptoms most associated with ovarian cancer: bloating, pelvic or abdominal pain, difficulty eating or feeling full quickly, and urinary symptoms such as urgency or needing to go more often.
Read that list and you will probably recognize sensations you have felt at some point. That is exactly the problem, and it is also the reason the medical guidance focuses less on the symptoms themselves and more on their pattern. According to the American Cancer Society, what raises concern is when these symptoms are new, persistent, and a clear change from what is normal for you, occurring more frequently or more intensely than usual. As a general guide, the organization notes that symptoms appearing more than roughly a dozen times in a month warrant a conversation with a doctor, and persistent urinary urgency or frequency lasting more than a few weeks should be reported promptly.
The point is not to turn every bloated afternoon into a crisis. Most of the time, these sensations come from something ordinary and benign. The point is to notice change and to honor it instead of explaining it away. Women are practiced at minimizing their own discomfort, at being busy, at assuming it will pass. The pattern that matters here is the body saying something consistently, over weeks, in a way it did not before. That is the signal to make the appointment, describe what you are noticing plainly, and ask to be taken seriously. Knowing the symptoms is step one. Trusting yourself enough to act on a pattern is the harder, more important step.
Family History and the Role of BRCA Genes
The thread that connected Jeanne’s case to Chris’s survival was genetic, and this is where Evert’s advocacy has been most pointed. Some ovarian cancers are tied to inherited gene changes, the most well known being mutations in the BRCA1 and BRCA2 genes. These same genes are widely discussed in connection with breast cancer, but they meaningfully raise ovarian cancer risk as well. A woman who inherits a harmful BRCA variant carries a substantially higher lifetime risk than a woman in the general population, which is why this information can be genuinely life-changing rather than merely interesting.
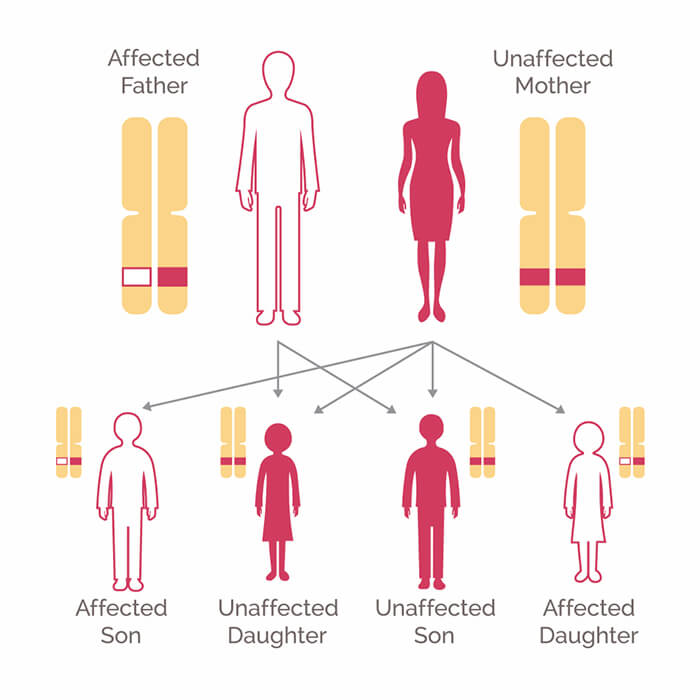
These variants run in families, and that is the crucial practical detail. A parent who carries a BRCA mutation has a roughly fifty percent chance of passing it to each child. A diagnosis in one relative, the way Jeanne’s became, can be the first clue that others in the family share the same elevated risk and do not yet know it. This is why family history is not a box to tick once and forget. It is living information that can shift as relatives are diagnosed, as genetic findings are reclassified, and as you learn more about the people whose biology you share.
Knowing your family history means more than knowing that “cancer runs in the family.” It helps to know which cancers, in which relatives, at what ages, and on which side. Ovarian, breast, and certain other cancers in close relatives can all be relevant. If your history raises questions, the appropriate next step is usually not to demand a screening test, but to ask your doctor whether a referral to genetic counseling makes sense. Evert reached her own diagnosis through exactly this kind of cascade, one family member’s information illuminating the path for another.
Genetic Counseling, Screening for Higher Risk, and Talking to Your Doctor

Genetic counseling deserves more attention than it usually gets, because people often imagine it as a single blood test with a yes-or-no answer. It is more thoughtful than that. A genetic counselor reviews your personal and family history, helps you understand what testing can and cannot tell you, walks through the implications of a result for you and your relatives, and helps you weigh decisions without pressure. Testing is a choice, and counseling exists to make that choice an informed one rather than a frightened one.
For women found to be at high risk, such as those who carry a BRCA1 or BRCA2 mutation, the calculus around monitoring changes. While routine ovarian cancer screening is not recommended for average-risk women, women at high risk may be offered periodic monitoring and a range of risk-reducing options, which can include preventive surgery of the kind Evert chose. These are deeply personal decisions made in partnership with specialists who can weigh a woman’s age, family plans, risk level, and values. There is no single right answer that applies to everyone, which is exactly why these conversations belong in a doctor’s office and not in a search bar.
For everyone else, the most useful tool remains an honest, ongoing relationship with a healthcare provider. That means describing symptoms accurately, mentioning family history even when no one asks, and asking direct questions: Given my history, is genetic counseling something I should consider? Is what I am feeling worth investigating? Self-advocacy is not about being difficult or anxious. It is about being a full participant in your own care, which is the role Evert has used her platform to encourage women to claim.
What Chris Evert Keeps Choosing to Make Public
The most striking thing about Evert’s involvement is that she did not have to share any of it. A retired champion is entitled to private medical care and a quiet life. She has instead spoken openly across more than one recurrence, having been diagnosed again after her first treatment, continuing to talk candidly each time about stepping back from commitments to focus on her health while staying, in her own framing, optimistic. Throughout, her message to other women has stayed consistent with what she wrote when she first went public: be your own advocate, know your family’s history, stay aware of your body, follow your instincts, and do not assume a worrying sign will simply pass.
That message lands with particular force because of who is delivering it. Evert built her career on noticing small things, on discipline, on paying attention. The same attentiveness she once brought to an opponent’s footwork she now asks women to bring to their own bodies and their own family stories. It reframes self-advocacy not as worry or vanity but as a skill, a learnable habit of attention that any woman can practice. Her openness about a genetic finding, a preventive surgery, and an early diagnosis turns a private medical history into a kind of public service, the sort that may quietly send a woman to ask her aunt how old she was when she was diagnosed, or to finally mention that persistent bloating at her next appointment.
If there is one thing to carry from her example, it is that the most powerful health tool available to most women is not a machine or a lab result. It is knowing your own story, knowing your family’s, and being willing to speak up before you can prove anything is wrong. Evert acted on a sister’s legacy and a piece of information she could easily have set aside, and that choice is the heart of what she keeps asking of the women who hear her.
This is a sensitive health topic, and if anything here has left you concerned about your own health or your family’s history, please reach out to a doctor or qualified healthcare professional who can guide you with care.