
By 3 p.m. her jeans wouldn’t button. She’d eaten a salad with grilled chicken at 12:30, drunk a glass of sparkling water, taken one bite of a coworker’s birthday cake out of politeness, and now the waistband she’d snapped shut at breakfast was leaving a red welt across her stomach. She was 38, healthy by every external measure, and quietly furious that nobody could tell her why her gut had decided, at some point in the last two years, that food was the enemy. Her gastroenterologist had ordered the usual panel, told her the labs were fine, and suggested she try to manage her stress. She left the office wondering if “fine” was just the medical word for “we didn’t look hard enough.”
Her story is one of the most common stories in women’s health, and it almost never gets named correctly. The gut isn’t just a digestive tube. It’s an endocrine organ, an immune organ, and a neurological organ, with more nerve endings than the spinal cord and a microbial population that outweighs the human cells it lives among. When that system goes sideways, the signals can show up almost anywhere in the body except where most clinicians are looking. The list below is the one a smart functional gastroenterologist would walk through. None of these signals are normal. All of them are treatable.
The Bristol Stool Chart Belongs in Every Bathroom
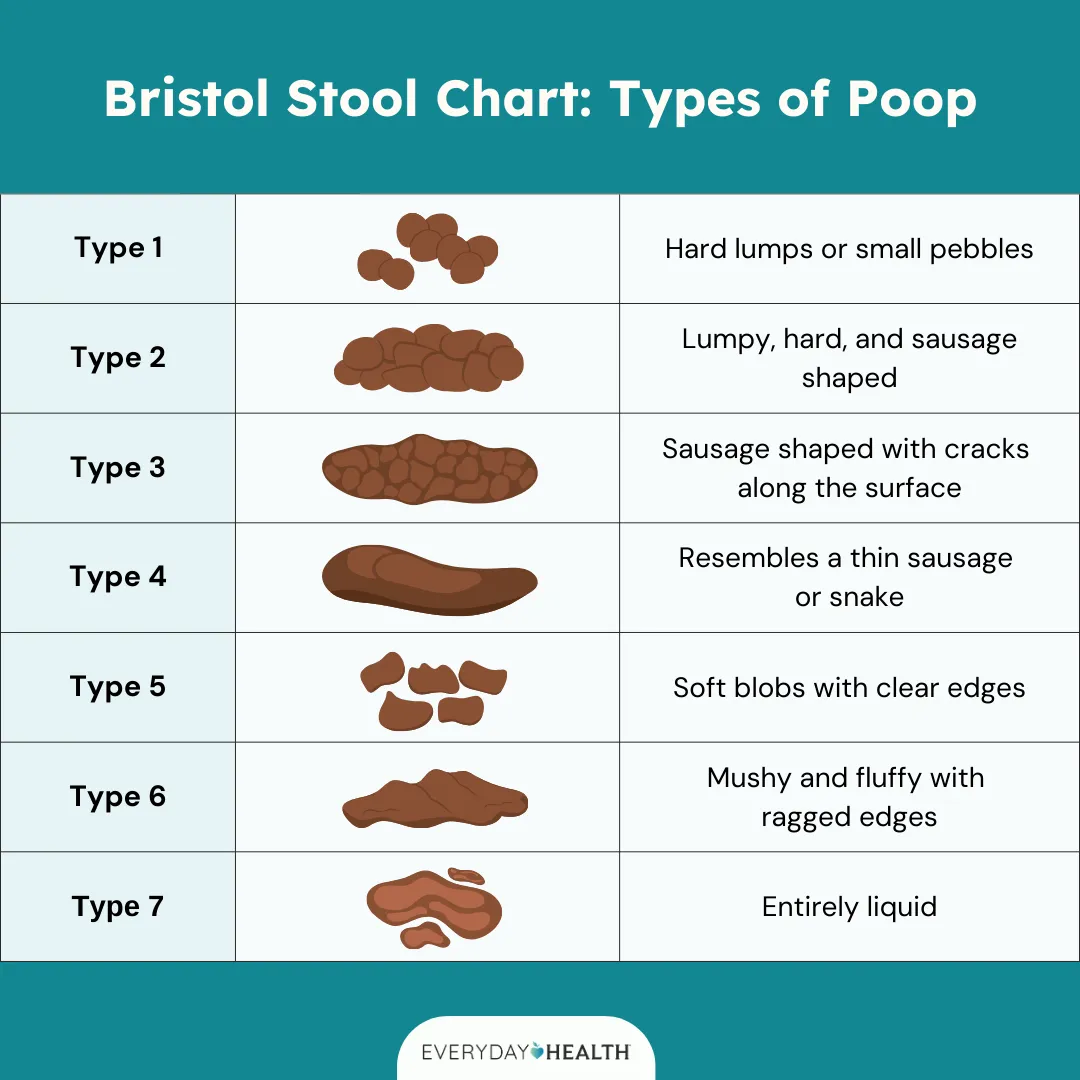
Before the symptoms get exotic, the single most useful gut diagnostic in the world is something a woman can do, alone, in 90 seconds, every morning. The Bristol Stool Chart, developed at the Bristol Royal Infirmary in 1997 and now used in clinical research across the globe, classifies stool into seven types. Type 1 is hard pebbles. Type 2 is a lumpy sausage. Type 3 is a sausage with cracks. Type 4 is a smooth, soft sausage. Type 5 is soft blobs with clear edges. Type 6 is mushy with ragged edges. Type 7 is liquid.
Healthy stool, the kind that signals a well-fed microbiome and an unhurried transit time, sits at Type 3 or Type 4. Type 1 and Type 2 mean constipation, slow transit, and often not enough fiber or water. Type 5 through 7 mean inflammation, food intolerance, dysbiosis, or in some cases an infection that nobody has thought to look for. Dr. Robynne Chutkan, an integrative gastroenterologist and author of Gutbliss , has spent two decades arguing that the chart belongs on the back of every bathroom door. The data she has on her own patients is striking. Women who track their type for two weeks come back with a clearer picture of what is wrong than most lab panels can produce.
Chronic Bloating Is Not a Personality Trait

Bloating that arrives within an hour of eating, sits like a balloon under the ribs, and resolves overnight only to come back the next afternoon is one of the most under-investigated symptoms in primary care. Women hear, again and again, that bloating is just a normal part of being a woman, especially after 35. It is not. Chronic daily bloating points to one of three things in most cases: a bacterial overgrowth in the small intestine called SIBO, a yeast overgrowth in the gut, or a food intolerance the body has not been screened for.
The perimenopause overlap is the part that gets missed. Falling progesterone slows gut motility, which lets bacteria sit longer in the small intestine, which feeds the overgrowth that drives the bloat. Estrogen volatility further inflames the gut lining. A woman who never had digestive trouble in her twenties can find herself, at 40, bloated every afternoon and unable to figure out which food triggered it because all of them seem to. Dr. Mary Claire Haver has flagged this perimenopausal gut shift as one of the most consistent patterns she sees in clinic, and it is almost never on a standard gastroenterology workup.
Morning Fatigue Versus Afternoon Fatigue

Where the fatigue lives on the clock is a clue. Fatigue that is heaviest in the morning, the kind that makes a 7 a.m. alarm feel cruel even after eight hours in bed, tends to point upstream of the gut, toward the adrenals, the thyroid, or sleep architecture. Fatigue that lands like a brick at 2 or 3 in the afternoon, the kind that arrives an hour or two after lunch and feels almost narcotic, points downstream into digestion. The food is not being processed cleanly. The blood sugar is spiking and crashing, or the gut is mounting an inflammatory response to something on the plate.
The pattern matters because the fix is different. Morning fatigue responds to cortisol support and a protein-rich breakfast within an hour of waking. Afternoon fatigue responds to a structured elimination diet, a fiber audit, and in some cases a SIBO workup. Dr. Will Bulsiewicz, a board-certified gastroenterologist and author of Fiber Fueled , frames the afternoon crash as the most reliable gut signal a woman can track without any equipment. If lunch consistently produces a slump within two hours, the gut is the system to examine.
Brain Fog After Eating

The gut-brain axis is no longer a wellness slogan. It is a documented neurological reality, with the vagus nerve running a direct line between the two organs and the gut microbiome producing roughly 90 percent of the body’s serotonin and a meaningful share of its dopamine. When the gut is inflamed, the brain hears about it within minutes. The clinical name is postprandial cognitive impairment, and it shows up as the kind of foggy, slow, slightly disoriented feeling that arrives 30 to 90 minutes after a meal and makes it hard to write a coherent email.
Dr. Mark Hyman, founder of the Cleveland Clinic Center for Functional Medicine, has spent years arguing that brain fog after meals is one of the clearest signals of food intolerance and gut inflammation that a woman can self-track. The mechanism is straightforward. Inflammatory cytokines released in the gut cross into circulation, the blood-brain barrier becomes more permeable under inflammation, and the brain registers the chemical noise as a slow, muddy cognition. The food driving it is almost always gluten, dairy, eggs, soy, corn, or sugar, and almost always one a woman is eating daily without thinking.
Sudden Food Intolerances After Years of Tolerance
The gut a woman has at 25 is not the gut she has at 40. Foods that produced no symptoms for a decade can begin, seemingly overnight, to produce bloating, fatigue, congestion, or skin reactions. This is not a sign that the body has become “weak.” It is a sign that the gut lining has lost some of its integrity, that the immune system at the gut wall has become reactive, or that the microbial population has shifted in a way that no longer tolerates what it used to tolerate.
The most common late-onset intolerances are dairy, gluten, and eggs, in that order. Dr. Robynne Chutkan describes a typical case as a woman in her late thirties who can no longer drink her morning coffee with cream without feeling congested, foggy, and bloated by noon. The fix is rarely permanent abstention. It is a 30-day elimination, a strategic reintroduction, and a parallel effort to repair the gut lining so that tolerance can be rebuilt. Skipping the repair step is the part that turns a temporary sensitivity into a lifelong restriction.
Recurring Adult Acne That Tracks With the Gut
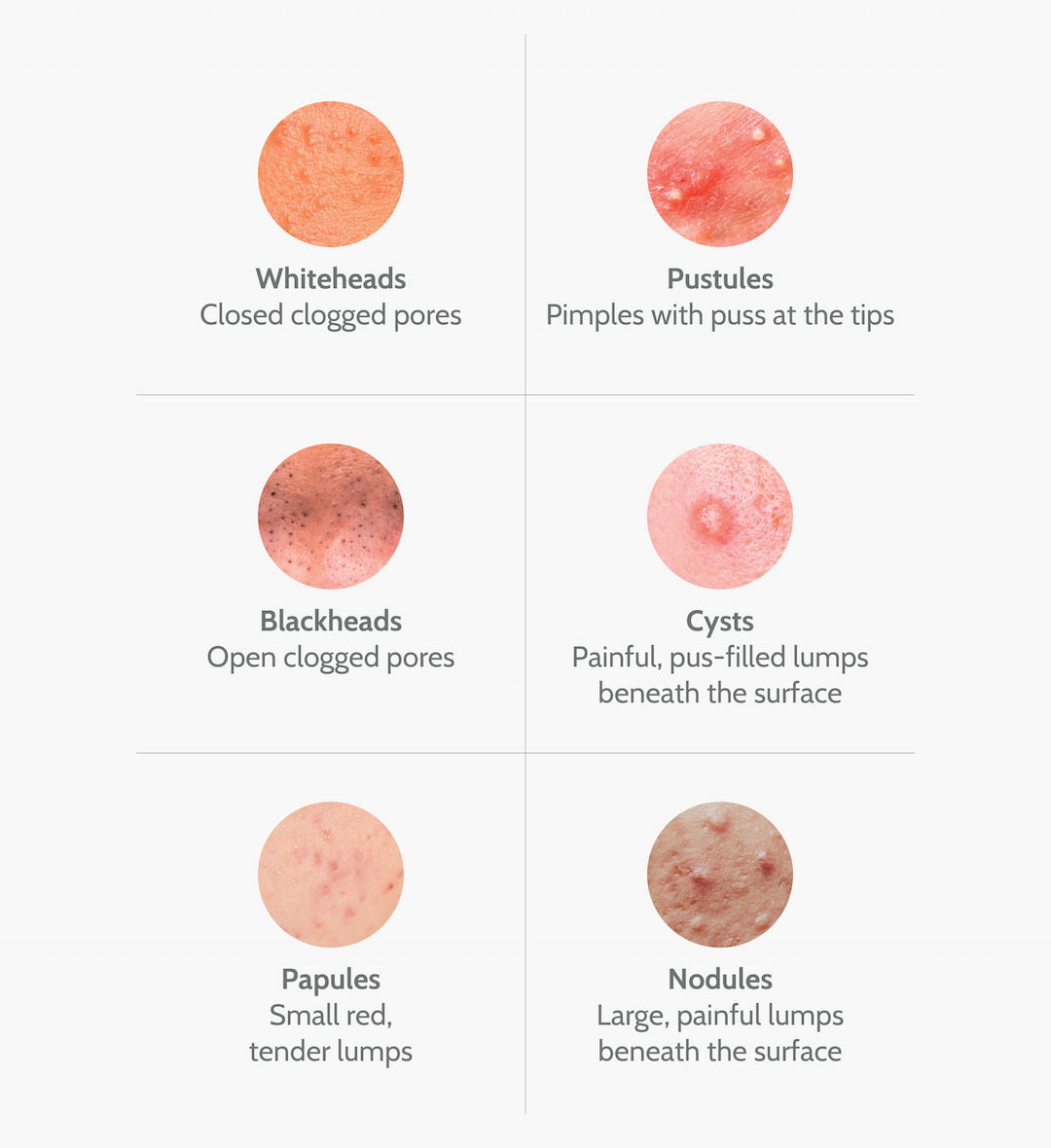
Acne in the thirties and forties is almost never a skincare problem. The face is a mirror of the gut, and adult acne, especially around the jawline and chin, correlates tightly with three gut-driven inputs: dysbiosis in the gut microbiome, food intolerances that drive systemic inflammation, and hormonal shifts that the liver and gut are no longer clearing efficiently. Dermatologists who treat with topicals alone often fail their adult patients for exactly this reason. The trigger is two organs away from the breakout.
The pattern to watch for is acne that flares 24 to 72 hours after a specific food, that clusters around the cycle, or that improves dramatically during a structured elimination diet. Dairy is the most frequent culprit, with studies in the Journal of the American Academy of Dermatology consistently linking dairy consumption to adult acne severity. Sugar and refined carbohydrates spike insulin, which drives androgens, which drives sebum production. A 30-day elimination of dairy and added sugar is, for many women, more effective than a topical retinoid prescription.
The 30-Day Elimination Protocol

The single most powerful diagnostic tool a woman can run on her own gut is a structured elimination diet. The protocol is unglamorous and works. For 30 days, remove dairy, gluten, and eggs completely. Read every label. Watch for hidden gluten in soy sauce and salad dressing, and hidden dairy in protein bars and processed foods. At the end of 30 days, reintroduce one food at a time, in larger-than-normal amounts for two consecutive days, and then return to the elimination diet for 72 hours while tracking symptoms.
The reintroduction is the diagnostic part. A clean reintroduction means no return of bloating, fatigue, brain fog, congestion, joint pain, or acne. A reactive reintroduction means symptoms surface within 72 hours, and the food can be filed as a known trigger. Many women discover that one of the three is fine and another is the entire problem. The clarity from a single 30-day cycle is often greater than the clarity from a year of guessing. A simple tracking journal, even something like a basic food and symptom journal , makes the pattern visible in a way memory alone cannot.
The Fiber Audit, 30 Grams a Day From Real Food

The average American adult eats 15 grams of fiber a day. The figure the gut microbiome actually needs to thrive sits at 30 grams or higher, and Dr. Will Bulsiewicz has built a career on the data showing that fiber diversity matters as much as fiber quantity. His American Gut Project research, published in mSystems , found that people who ate 30 or more different plant foods a week had a measurably more diverse and resilient microbiome than people who ate 10 or fewer, regardless of whether they identified as vegetarian or omnivore.
A fiber audit is a one-week exercise. Track every plant food eaten, by name, for seven days. Count beans, lentils, nuts, seeds, whole grains, vegetables, fruits, herbs, and spices. The number that comes back is usually startling. Most women land between 12 and 18. The fix is to add, not subtract: a daily smoothie with three plants, a soup with five plants, a salad with seven plants, a stir-fry with six plants. Fiber from real food, not from a powdered supplement, is the input that feeds beneficial bacteria and produces the short-chain fatty acids that heal the gut lining.
Fermented Foods Earn Their Place

A daily serving of fermented food is one of the most evidence-backed gut interventions in nutritional science. A Stanford study published in Cell in 2021 followed two groups of adults for ten weeks, one eating six servings of fermented food a day and one eating a high-fiber diet. The fermented food group showed a significant increase in microbial diversity and a measurable decrease in 19 inflammatory markers. The high-fiber group showed benefits too, but the speed and breadth of the fermented food group surprised the researchers.
The fermented foods that matter are the ones with live cultures: kimchi, sauerkraut, kefir, yogurt with live active cultures, miso, and tempeh. Kombucha is fine but lower in beneficial bacteria than the others. A reasonable daily target is two tablespoons of kimchi or sauerkraut at lunch and a small glass of plain kefir in the morning. The fermented food has to be refrigerated and unpasteurized, which means the shelf-stable jar of “sauerkraut” in the canned goods aisle does almost nothing. The refrigerated section is the only one that counts.
Probiotic Strain Matters More Than Brand
The probiotic aisle is a marketing landscape, not a clinical one. Brand names and CFU counts dominate the labels, while the actual strain, which is the part that determines what the probiotic does, is buried in small print. A probiotic is only as useful as the strain inside it, and the strain has to match the condition being treated.
For irritable bowel symptoms with bloating and altered stool, the evidence points to Lactobacillus rhamnosus GG and Bifidobacterium infantis 35624, the latter studied extensively in the American Journal of Gastroenterology . For traveler’s diarrhea and antibiotic-associated diarrhea, Saccharomyces boulardii has the strongest data and is technically a beneficial yeast rather than a bacterium. For women with recurrent yeast or urinary tract infections, Lactobacillus reuteri RC-14 and Lactobacillus rhamnosus GR-1 have specific clinical research behind them. Generic “multi-strain” probiotics with 50 billion CFU and no named strains are usually a waste of money. A strain-specific option like Florastor with Saccharomyces boulardii is one example of a clinically targeted product. The principle holds across the category: read for the strain, not the marketing.
Bone Broth and the Gut Lining

The gut lining is a single layer of cells, one cell thick, with tight junctions holding them together. When those junctions loosen, a condition increasingly recognized in research literature as increased intestinal permeability, partially digested food and bacterial byproducts cross into circulation and drive the systemic inflammation that shows up as fatigue, brain fog, joint pain, and skin issues. Repairing the lining is not optional. It is the foundation of any gut protocol.
Bone broth, made from bones simmered for 12 to 24 hours, delivers collagen, glutamine, glycine, and proline, the building blocks the gut lining uses to repair itself. A daily cup, taken in the morning or as a between-meal sip, supports that repair. Glutamine in particular is the preferred fuel for the cells that line the small intestine. For women who do not have time to simmer a stockpot for 24 hours, a clean powdered version such as a grass-fed bone broth protein powder delivers the same amino acid profile. The repair window is six to twelve weeks of consistent intake, paired with the elimination of the foods that were inflaming the lining in the first place.
When to Push for a SIBO Breath Test or a GI-MAP

If a 30-day elimination, a fiber audit, daily fermented foods, a targeted probiotic, and a gut-lining repair protocol have not resolved the symptoms after three months, the next step is testing. The two tests worth knowing about by name are the SIBO lactulose breath test and the GI-MAP stool test, neither of which is part of a standard gastroenterology workup.
The SIBO breath test measures hydrogen and methane gases produced by bacteria in the small intestine after a sugar challenge. Elevated hydrogen at 90 minutes points to bacterial overgrowth that drives bloating, while elevated methane points to a slower-transit variant linked to constipation. The GI-MAP is a DNA-based stool test that maps the gut microbiome, screens for pathogens like H. pylori and parasites, and measures markers of inflammation and digestive function. A standard gastroenterologist will rarely order either one. A functional medicine practitioner, a naturopath with gastrointestinal training, or an integrative GI like Dr. Chutkan will. The cost is real, often between 300 and 500 dollars out of pocket, and the diagnostic clarity is often worth it after months of guesswork.
The Bigger Picture

The gut is the system that connects everything else. It feeds the immune system, regulates the brain, processes the hormones, and decides which nutrients the rest of the body gets to use. When it goes sideways, the symptoms scatter so widely that no single specialist sees the pattern. The dermatologist treats the acne. The neurologist looks at the brain fog. The endocrinologist looks at the fatigue. The gastroenterologist looks at the bloating. Nobody adds it up.
The woman who couldn’t button her jeans at 3 p.m. eventually ran the protocol. Thirty days off dairy, gluten, and eggs. A daily fiber count that climbed from 14 grams to 32. A small jar of kimchi in the fridge that she dipped into at lunch. A strain-specific probiotic with Bifidobacterium infantis. A cup of bone broth in the morning. By week three, the afternoon bloat had thinned. By week six, the brain fog was gone. By week ten, she reintroduced eggs cleanly, found dairy was the entire problem, and rebuilt her routine around that single piece of information. None of it required a prescription. All of it required a clinician, even a self-appointed one, willing to ask the right questions of a system that had been quietly trying to communicate for years. That kind of clinician sometimes shows up in a white coat, and sometimes shows up in your own bathroom on a Tuesday morning with a notebook.