It was a Wednesday afternoon in October 2024, the kind of late-fall Atlanta day where the air had finally cooled and the dogwood outside the office window had started to turn copper, and I was sitting on the paper-covered exam table at a primary care office in Brookhaven trying to describe what had been happening to my chest. Palpitations. Three or four times a week. Sometimes when I was sitting on the couch, not climbing stairs, not even reaching for a glass of water. I had written notes in my phone for two weeks before this appointment so I could be exact about it. The new patient form had asked me to rate my symptom severity on a one-to-ten scale and I had circled six and added a sentence in the margin. The doctor walked in, looked at the intake sheet, looked at me, and the first complete sentence he said to me was about my BMI. The second sentence was that we should “address that first before chasing anything else.” The third sentence was “lose twenty pounds and see if the palpitations resolve.” He had not listened to my heart. He had not asked when the palpitations started. He had not asked about my family history of arrhythmia, which is significant and which I had written on the form. I walked out of that office twenty-three minutes after I walked in, sat in my car in the parking deck, opened the Notes app, and wrote one sentence at the top of a fresh page. “I am building the list differently now.”
That list is the reason this article exists. What I did between October 2024 and the spring of 2025 was systematically rebuild how I found doctors. I stopped using insurance portals as my starting point. I stopped relying on word-of-mouth from women whose bodies looked nothing like mine. I built a process, with directories that actually exist, scripts that actually work in an exam room, and a set of rules for when to stay and when to leave. I have walked maybe two dozen plus-size women through this process in the year since, and the framework is durable enough now that I want to put it in print. If you have ever been told your symptom is your weight before the doctor heard the symptom, this is for you. If you have ever postponed a Pap smear or a thyroid check because the appointment itself is the thing you are most afraid of, this is for you. If you have a daughter, a sister, a wife who has told you the doctor’s office is the place she dreads more than any other room in her life, hand her this. The work of finding a doctor who will treat you as a person before they treat you as a body mass index is real work, and it is doable, and you do not have to invent the playbook from scratch.
The medical-fatphobia research (named studies, real numbers)
The first thing to understand is that what happened in that Brookhaven exam room is not a one-off. It is a measurable, replicated pattern in the peer-reviewed literature, and the literature is now substantial enough that it cannot be dismissed as anecdote. Sean Phelan and colleagues published a 2015 review in Obesity Reviews titled “Impact of weight bias and stigma on quality of care and outcomes for patients with obesity” that pulled together the evidence on what providers actually do when they see a fat patient. The pattern across studies is consistent. Providers spend less time with higher-weight patients. They build less rapport. They are less likely to refer for further diagnostic testing. They attribute symptoms to weight at a higher rate, and they do this before completing the standard differential diagnosis a thinner patient would receive. That is not a moral failing of individual doctors. It is a systemic pattern visible in the data.
The Phelan paper matters because it gave clinicians the citation they needed to start talking about this internally. The earlier work that opened the door is Angelina Sutin and Antonio Terracciano’s 2013 paper in
PLOS One
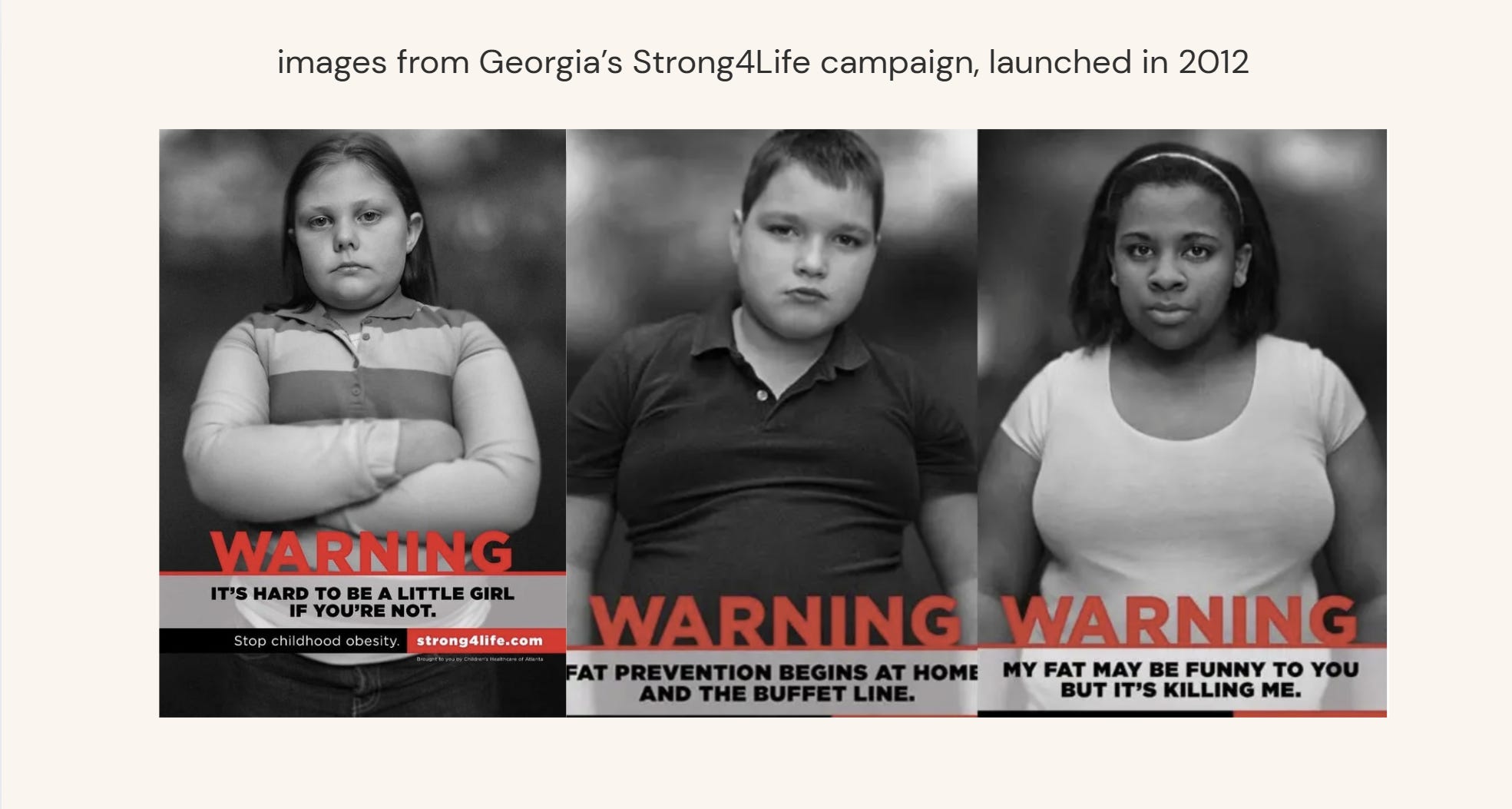
, “Perceived weight discrimination and obesity,” which followed a cohort of more than six thousand adults across two waves of the Health and Retirement Study and found that experiencing weight discrimination was associated with a meaningfully higher risk of remaining at higher weight, controlling for all the variables you’d expect. The takeaway, which the authors stated plainly, is that the stigma itself does not produce the behavioral change clinicians were assuming it produced. The stigma produces avoidance. Of doctors. Of gyms. Of food eaten in public. Of the very behaviors the stigma is theoretically supposed to incentivize. The intervention does not work, the intervention causes harm, and the data has been clear about this for over a decade.
Aubrey Gordon, in her 2020 book “What We Don’t Talk About When We Talk About Fat,” compiles the lived-experience side of this with a level of citation most popular books in this space do not bother with. Her chapter on healthcare is the one I have given as a printed photocopy to more women than any other piece of writing on this topic. Gordon names the specific mechanism. The fat patient walks in with a symptom. The doctor sees the body before they hear the symptom. The symptom gets recoded as a weight issue, which means the symptom does not get investigated, which means the actual underlying condition - the gallstones, the thyroid, the cardiac, the endometriosis - goes undiagnosed for months or years longer than it would in a thinner patient. Gordon names women who died from delayed diagnoses where the chart, in retrospect, showed the relevant symptom flagged at multiple visits and dismissed as weight. The book is not theoretical. The book has names in it.
Dr. Joshua Wolrich, an NHS surgeon in the UK whose 2021 book “Food Isn’t Medicine” is the most accessible introduction to the actual evidence on weight and health that I have found, makes the medical case from inside the profession. Wolrich’s argument is that the equation of weight with health is bad science, that BMI was never designed as a clinical diagnostic tool (Adolphe Quetelet developed it in the 1830s as a population-level statistical measure, not an individual one), and that the practice of using BMI as a gatekeeping mechanism for further investigation is one of the more damaging legacies of twentieth-century medicine. He is not an outlier. He is a working surgeon writing what the data already shows. The reason his book matters for plus-size women is that he gives you the citations to hand a skeptical doctor. The conversation in the exam room goes differently when you can cite Wolrich citing the underlying meta-analyses than when you are arguing from feeling.
Dr. Sand Chang, an Oakland-based psychologist who has worked with Stanford counseling services and Kaiser Permanente Transgender Services and is one of the most cited voices in HAES-aligned mental health care, has done the work of connecting medical fatphobia to its compound effects on patients who are also queer, trans, disabled, or fat at the intersection of multiple marginalizations. Chang’s clinical writing and conference work through HAES-aligned channels and the Association for Size Diversity and Health makes the case that the experience of being a fat patient isn’t separable from the other axes a patient is being read along. The trans plus-size patient does not experience medical fatphobia and transphobia as two separate events. They experience a single compound exposure that doubles or triples the rate of substandard care. I will return to this in a dedicated section because it deserves more than a sentence.
The research, in aggregate, gives you three things you can bring into an exam room. First, you can name the pattern. The dismissal of your symptom as a weight issue is not personal, it is documented, and it is wrong. Second, you can cite the work. Phelan 2015 and Sutin 2014 are the two names to remember if you ever need to push back with a doctor who claims this is “just political.” Third, you can stop blaming yourself for the avoidance. If you have postponed appointments for months or years because of how doctors have treated you, that is a documented response to a documented pattern. The avoidance is not your weakness. It is your nervous system telling you the room was not safe.
The 4 directories that actually work
The directory question is the one I get asked most often, and the honest answer is that no single directory covers every zip code in the United States. What works is using four of them together, cross-referencing, and accepting that for many people the first usable name is going to be a telehealth provider until a local option opens up. The four I trust enough to send women to are below, in the order I would use them.
The first is the Association for Size Diversity and Health (ASDAH) Health At Every Size practitioner list. ASDAH is the organization that holds the HAES framework, and their directory is the closest thing to a vetted national list of providers who have signed onto the principles. The principles themselves are public on the ASDAH site and worth reading in full before you start the search, because they tell you what a HAES-aligned provider is committing to. The list itself is searchable by state and by specialty. The limitation is that it covers practitioners who have actively opted in, which means a doctor in your zip code who practices weight-inclusive medicine but has not signed up will not appear. Use it as a floor, not a ceiling. The web address moves periodically, so I will say only that searching “ASDAH HAES practitioner directory” will get you there.
The second is the Center for Body Trust provider directory (formerly Be Nourished), run out of Portland by Hilary Kinavey, a licensed professional counselor, and Dana Sturtevant, a registered dietitian, who together built the Body Trust framework starting in 2005. Their directory leans heavier on therapists and dietitians than on MDs, but their listings are higher-vetted than ASDAH’s because providers go through a Body Trust certification process before they appear. If you are looking for a HAES-aligned therapist or RD in addition to an MD, Be Nourished is the better starting point. For OB-GYN and PCP specifically, you will still need to cross-reference with ASDAH or Plus Size Birth.
The third is the Plus Size Birth provider list, curated by Jen McLellan, who has been doing public-facing plus-size pregnancy and birth work since 2013. McLellan’s directory is the most operationally useful one I know of if you are pregnant, trying to conceive, or in active OB-GYN care. The reason is that she screens for specific behaviors. Does the provider use weight-inclusive language in their intake. Do they have appropriately sized blood pressure cuffs and exam gowns. Do they refuse to weigh you on request without making it a fight. The screening criteria are listed on her site. Even if you do not find a provider in your zip code, McLellan’s site is worth reading for the questionnaire she uses to evaluate them, which you can adapt for your own search.
The fourth is the curated reading work of Sonalee Rashatwar, the licensed clinical social worker and sex therapist known publicly as The Fat Sex Therapist. Rashatwar’s referral lists are not a formal directory in the same way the others are. They are recommendations across her published work and her social presence, often pointing to specific named providers in specific cities. The reason her network is useful is that she works at the intersection of fat liberation, queer health, and trauma-informed care, and the providers she points to have usually been vetted through that triple filter. If you are queer, fat, and have a trauma history with medical care, Rashatwar’s named referrals are often the first place a usable doctor surfaces. Her work also explicitly addresses the South Asian and broader diaspora plus-size community, which most other directories do not.
Two honorable mentions that I use as cross-reference layers. The Body Positive Therapist Directory, maintained by Connie Sobczak and Elizabeth Scott’s Body Positive organization, is mental-health-focused but worth searching if you want a therapist who will not pathologize your body. And the Size Friendly Care lists curated by various HAES-aligned advocates - including some of Rashatwar’s network - circulate in fat-liberation spaces and occasionally surface specific providers who do not appear in the formal directories. Search for them, but verify everything. A name on an informal list is a lead, not a credential.
How to vet a doctor before the first visit (questionnaire)

The directories give you names. They do not tell you, before you walk in, whether the office itself will treat you well. The vetting work happens between finding the name and booking the appointment, and it is the step most women I work with skip because it feels confrontational. It is not confrontational. It is administrative. You are gathering information that any consumer of any service is entitled to gather. The phone call to the front desk before you book is the first filter, and a good one.
The call sounds like this. “Hi, I am considering becoming a patient and I have a few questions before I book. Do you have a weight-inclusive or HAES-aligned approach to care. Do you have blood pressure cuffs sized for larger arms and exam gowns sized over 2X. Is it possible to decline being weighed at visits when weight is not clinically necessary for the appointment.” Three questions. Each one tells you something. The pause before the answer tells you almost as much as the answer. A front desk that has heard the questions before will have a clean reply. A front desk that has not will get defensive or confused. Both are data.
The deeper vetting happens through the office’s online presence. Look at the provider’s bio for language clues. Words like “weight management,” “obesity medicine,” and “weight loss counseling” in the practice description are flags. Not always disqualifying, but flags. Words like “body diversity,” “weight-inclusive,” “HAES,” “intuitive eating,” or “non-diet approach” are positive signals. If the practice has a patient portal you can preview, check whether the intake forms ask for weight as a first-line data point or whether they ask about it contextually. The forms are written before you walk in, and they tell you what the practice considers central.
Reviews are useful but read them with a filter. Plus-size women leave reviews using a specific vocabulary that other patients do not. If you see reviews mentioning “the doctor actually listened,” “did not blame my weight,” “took my pain seriously,” those are usually from plus-size or chronic-pain patients who have learned to signal this carefully. Conversely, reviews celebrating a doctor for being “honest about my weight” or “telling it like it is” are usually a warning. The vocabulary tells you who the practice serves well.
The final pre-visit step, which I now do for every new provider, is sending a pre-visit email. I will give you the template in the next section. The purpose of the email is to surface the obvious flags before you have invested the copay and the time. If the provider’s response is gracious, the appointment is likely to go well. If the response is dismissive or defensive, you have saved yourself a wasted visit. Some providers will not respond at all, which is its own answer.
The pre-visit email template (copy-paste version)
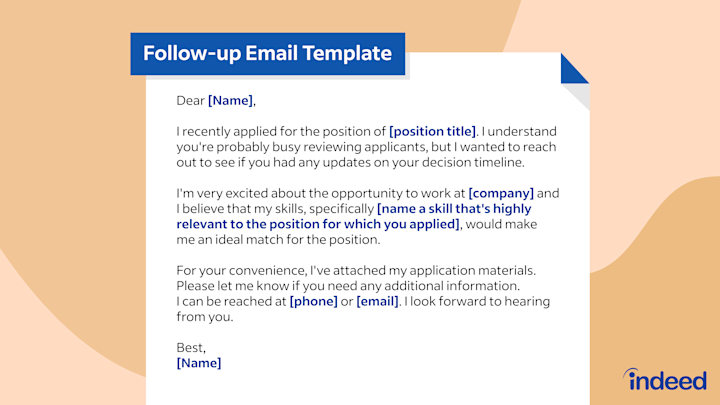
Here is the email I send. You can copy it verbatim, change the specifics, and adapt the symptom to whatever you are actually coming in for. It runs about one paragraph because longer emails do not get read by front-desk staff and shorter emails do not surface the actual information you need.
Subject line: New patient inquiry, [your name], approach to weight-inclusive care
“Hello, my name is [first and last] and I am considering Dr. [last name] as my new primary care provider [or OB-GYN]. Before booking, I wanted to share a few things about how I prefer to engage with care. I follow a weight-inclusive approach to my own health, and I have had past experiences where symptoms were attributed to my weight before being investigated, which led to delayed diagnoses. I would prefer not to be weighed at appointments unless weight is clinically necessary for the specific issue being addressed, and I would like any weight-related conversation to be patient-initiated rather than provider-initiated. The reason I am coming in is [specific symptom or screening, in one sentence]. Can you let me know whether this approach is one Dr. [name] is comfortable with, and whether the practice has appropriately sized blood pressure cuffs and gowns. I appreciate your time and look forward to hearing back.”
That is it. Three pieces of information conveyed. Your approach. Your specific symptom. Your operational needs. The email does the work of filtering before the appointment. I have sent this email maybe forty times over the last fifteen months. About a third of practices respond warmly and the appointment proceeds. About a third respond non-committally, which I read as a yellow flag and either skip or proceed with low expectations. About a third do not respond at all, which I now treat as a hard no. The ones who do not respond before the visit do not respond well during the visit either. The correlation is high enough that I trust it.
The 4-sentence opener for the exam room
The pre-visit email is the asynchronous layer. The 4-sentence opener is the live exam-room layer, and it is the single most important script in this article. The opener is what you say after the provider walks in, after the small talk about the weather, after they ask “so what brings you in today.” The reason it is four sentences and not three or five is that four is the length that fits inside the average attention span of a doctor in a fifteen-minute slot. Three is too short to convey context. Five gets interrupted. Four is the sweet spot.
The opener: “I want to start by naming that I take a weight-inclusive approach to my own health, and I would prefer that we not discuss my weight today unless it is clinically necessary for the issue I am here about. The issue I am here about is [specific symptom, with a duration and a frequency]. Here is what I have noticed and what I have already tried [one sentence of context]. What I am hoping for from this visit is [specific diagnostic or referral ask].” Four sentences. Memorize them. Practice them in the car before you walk in. The reason to memorize is that the moment a doctor sits down and looks at your chart is the moment your nervous system is most likely to go quiet on you. Having the sentences pre-loaded means you do not have to compose under pressure.
The opener works for two reasons. First, it sets the frame of the visit before the provider sets it for you. Most exam-room dynamics are determined in the first sixty seconds by who establishes the agenda. If the doctor’s first move is to comment on your weight, the rest of the visit is spent recovering from that. If your first move is to name your approach, the visit proceeds on the terms you set. Second, the opener gives the provider a specific ask. Doctors are problem-solvers under time pressure. If you hand them a defined problem and a defined hoped-for outcome, they have something to work on. If you hand them only a symptom, the path of least resistance for an overworked clinician is to default to the BMI conversation because it is fast.
The opener fails in two ways. It fails if you deliver it apologetically, because the apology signals that you do not believe you are entitled to the request, and providers read that. Deliver it the same way you would tell a mechanic which sound the car has been making. Matter-of-fact. The opener also fails if you do not have the specific symptom ready. “I just have not been feeling well” is not a symptom. “Palpitations three to four times a week, lasting under a minute, often when seated, started in early September” is a symptom. The specificity is the leverage.
The BMI-pushback script (specific phrasing)
Even with the email and the opener, you are still going to hit the BMI conversation in some appointments. Not all. But enough that you need a script for it. The pushback script has three layers, and you use them in escalating order based on how the provider responds.
Layer one, when the provider first mentions BMI or weight in a context unrelated to your symptom. “I appreciate that you are bringing this up, and I want to circle back to the specific issue I came in for. Can we address [your symptom] first, and if weight is clinically relevant to that diagnosis, we can return to it after.” That sentence does three things. It does not deny the provider’s framing. It redirects to your agenda. And it concedes that weight could become relevant, which keeps you from sounding evasive. Most providers, hearing that, will accept the redirect.
Layer two, when the provider insists that weight must be addressed first or attributes your symptom directly to weight without diagnostic workup. “I hear that this is your assessment. Can you tell me what diagnostic steps you would take if I presented with these same symptoms at a lower weight, and can we proceed with those steps now, since the symptoms are what I am here to address.” That sentence is the most powerful one in this article. It does not argue about whether weight matters. It asks the provider to name the differential diagnosis they would run for a thinner patient. Most providers, when asked this directly, cannot defend giving you a different workup than they would give a thinner patient with the same presentation. The question makes the disparity visible.
Layer three, when the provider refuses to proceed with diagnostic workup and continues to insist on weight loss as the primary intervention. “I am going to ask you to note in my chart that I requested [specific diagnostic test or referral] and that you declined to order it. I would like a copy of that note for my records.” The chart note request is the legal lever. Once you say it, the provider has to either order the test, document the refusal, or both. Documented refusals show up later if you escalate to a complaint or pursue a malpractice review, and the provider knows that. In my experience, layer three is needed in maybe one out of five appointments where layers one and two failed. The other four times, layer two is enough.
When to demand a referral (specific symptoms)
There are specific symptoms where the default diagnostic workup is well-established in the literature and the failure to perform it on a higher-weight patient is documented enough that you should not accept dismissal. I will name the ones I see most often, with the referral or test you should be asking for.
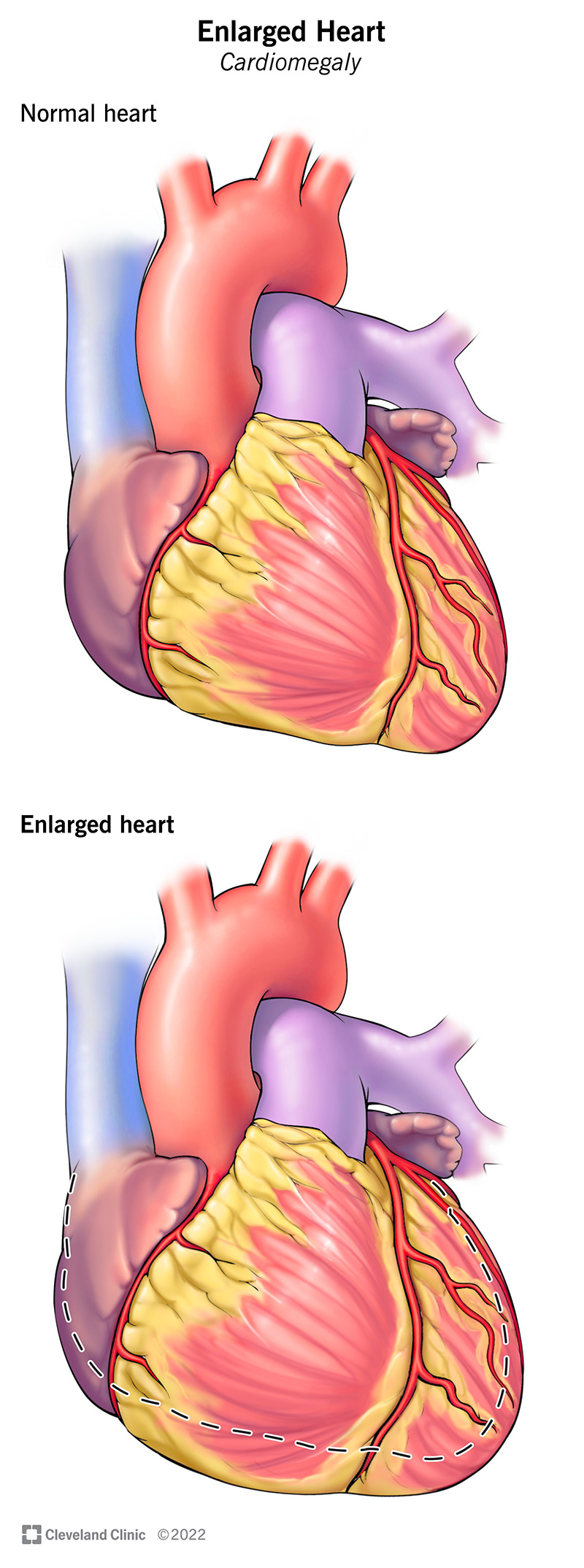
Heart palpitations, chest pain, or unexplained shortness of breath should produce an EKG at minimum and a referral to cardiology or a Holter monitor if symptoms persist. The dismissal pattern here is to attribute these to anxiety, deconditioning, or weight. The standard of care, irrespective of body size, is to rule out arrhythmia and structural cardiac issues first. If your provider declines to order an EKG for cardiac symptoms, that is a layer-three pushback moment.
Pelvic pain, heavy bleeding, painful sex, or irregular cycles should produce a pelvic exam, a transvaginal ultrasound, and a referral to OB-GYN if your PCP is not equipped to evaluate. The dismissal pattern is to attribute these to hormones, weight, or stress without imaging. The standard of care includes ruling out fibroids, endometriosis, ovarian cysts, polycystic ovary syndrome, and adenomyosis. None of those diagnoses correlate with weight in a way that lets a clinician skip the imaging.
Joint pain, especially knee or hip pain in someone under fifty, should produce imaging and a referral to orthopedics or rheumatology if persistent. The dismissal pattern is “lose weight and see if it helps.” The standard of care includes ruling out osteoarthritis, autoimmune arthritis, and bursitis with appropriate imaging. Weight loss may eventually be part of a treatment plan after diagnosis, but it is not the diagnosis.
Fatigue, especially when accompanied by hair loss, cold intolerance, weight changes, or mood changes, should produce a complete thyroid panel including TSH, free T4, free T3, and thyroid antibodies. The dismissal pattern is to order TSH alone and call it a workup. A complete panel is what catches subclinical hypothyroidism and Hashimoto’s, both of which are commonly missed in plus-size women because the TSH-only screen does not surface them.
Headaches that change in pattern, frequency, or severity, especially with visual changes, should produce a neurological exam at minimum and imaging if the exam is abnormal. The dismissal pattern is to attribute these to dehydration, stress, or screen time. The standard of care includes ruling out idiopathic intracranial hypertension, which is actually overrepresented in higher-weight women and gets missed because providers attribute the headaches to weight without performing the exam that would surface the actual diagnosis.
The rule across all of these is the same. The diagnostic workup for the symptom does not change because of your body size. If the workup is being skipped, the workup is being skipped, and the failure to perform it is the deviation from standard of care, not the request to perform it.
When to fire your doctor (the 3-strike rule)

The decision to leave a provider should not be made in the heat of one bad appointment. Most of us, when we have a bad visit, either over-react and burn the relationship or under-react and stay for years past when we should have left. The framework that has worked for me and the women I mentor is the 3-strike rule. Three documented incidents, of specific types, are the threshold for switching providers. Fewer than three means you give feedback and stay. Three or more means you go.
Strike one is any single instance of the provider attributing a symptom to weight before performing the standard diagnostic workup for that symptom. One instance is forgivable as a bad day, a missed cue, or a provider who responds when corrected. After the appointment, you write the follow-up letter (template in the next section), and you note in your records that you have documented the incident. If the provider acknowledges and corrects, strike one stands but does not escalate.
Strike two is a second instance of the same pattern, after the first has been raised. Two instances signal that the first was not a bad day but a default mode. At this point, you should already be researching alternatives and you should not invest in further attempts to coach the provider through it. Your job is not to train your doctor. Your job is to receive competent care.
Strike three is any instance where the dismissal results in delayed diagnosis or actual harm. If a symptom you flagged was dismissed as weight, and the symptom turned out to be a real underlying condition that was diagnosed later by a different provider, that is an automatic exit, regardless of strike count. You do not stay at a provider who has missed a diagnosis on you, even if they apologize.
The other auto-exit triggers, separate from the three-strike count, are any moment where the provider raises their voice at you, lectures you about food intake without your invitation, refuses to order a test you specifically requested without documenting the refusal, or makes any comment that crosses from clinical assessment into personal judgment of your character or self-worth. Any of those is a single-incident exit. You do not need to count to three.
The mechanics of leaving are simple. You request your medical records be transferred to your next provider, you send a brief written note thanking the practice and asking for closure of your file, and you do not engage in a debate about why you are leaving. If they ask for feedback in an exit survey, give it. If they do not, you owe them nothing. The energy you would spend on the exit conversation is energy you need for the search for the next provider, and the next provider is what matters.
Insurance and HAES providers: navigating coverage

The hardest practical part of all of this is that HAES-aligned providers are not evenly distributed across insurance networks. Many of them, especially the ones who have built their practice around this framework intentionally, are out of network for at least some major insurers, and some of them have moved to cash-pay or direct primary care models specifically to opt out of the volume-driven incentives that produce rushed appointments. The result is that you may find a doctor who is right for you and discover that your insurance does not cover them, or covers them at a higher coinsurance.
The options here are real but limited. First, use your insurance’s out-of-network benefit if you have one. Most PPO plans cover out-of-network providers at a reduced rate, and the difference between in-network and out-of-network may be smaller than the cost of staying with a provider who is missing diagnoses on you. Calculate it. The math sometimes surprises people.
Second, look at the practice’s payment structure. Some HAES-aligned PCPs run direct primary care models with a flat monthly fee, often between fifty and two hundred dollars a month, which includes unlimited visits and basic labs. If your usage is heavier than average - which it often is for women managing thyroid, PCOS, or autoimmune conditions - the math can favor direct primary care over conventional insurance plus copays. The direct primary care provider is also more likely to spend thirty minutes with you on a visit rather than fifteen, because their incentive structure rewards relationship rather than volume.
Third, if you are limited to in-network providers by financial necessity, do the directory work inside your network. Most insurers’ provider search tools let you filter by specialty and read provider bios. Look for the same language signals - weight-inclusive, body diversity, HAES, intuitive eating - in the bios of in-network providers. They are rarer but they exist. Cross-reference any candidate against ASDAH or the other directories to see if they are also listed there.
Fourth, telehealth has changed the math significantly. HAES-aligned providers offering telehealth across multiple states means that geographic isolation is less of a barrier than it was even three years ago. Dr. Lesley Williams, a board-certified family medicine physician at Mayo Clinic Arizona and a Certified Eating Disorder Specialist who has been one of the most public HAES-aligned MDs in the country, is one example of a clinician building care around weight-inclusive principles. Practices like hers are part of the network I point women to when they can’t find a local option. The first visit can be telehealth, and many of the diagnostic conversations can happen there even if certain follow-ups require an in-person visit eventually.
The follow-up letter template (when care goes wrong)
When a visit goes badly, the follow-up letter is the tool you reach for. The letter has three functions. It documents the incident in writing, which creates a paper trail. It gives the provider a chance to respond, which sometimes produces an apology and a corrected approach. And it preserves your own clarity about what happened, which is harder than it sounds because the memory of a bad appointment tends to soften within a day or two and you start to question whether it was really that bad. The letter is your present self telling your future self what was said.
Here is the template. Send it within seventy-two hours of the visit while the details are fresh, by patient portal message if your provider has one or by certified mail if they do not.
“Dear Dr. [last name], I am writing to document my visit on [date] and share some feedback. During the appointment, I came in to address [specific symptom]. The interaction included [specific quoted statement or specific behavior, as exact as you can remember]. This raised concerns for me because [the standard of care for this symptom is X, or you had previously requested weight not be the first lens, or the symptom was not investigated]. I would like to request [what you want now, whether that is the diagnostic test that was skipped, a referral, a note in your chart, or simply an acknowledgment]. I am sharing this directly with you rather than escalating to a complaint because I would prefer to give you the opportunity to address it. Thank you for your time.”
That letter, sent without anger and with specific details, produces one of three outcomes. The provider apologizes and corrects, which has happened to me three times out of maybe a dozen letters sent. The provider responds defensively or not at all, which tells you the exit decision is the right one. Or the practice’s office manager intervenes and the situation gets routed to a different provider within the practice, which is sometimes a workable outcome if you like the practice but not the specific doctor. All three outcomes are useful information.
If the dismissal resulted in actual harm - a missed diagnosis, a delayed referral that allowed a condition to worsen, a refusal that violated standard of care - the next step beyond the letter is a formal complaint to your state medical board. The threshold for this is higher and you should generally consult with a patient advocate or a malpractice attorney before filing. Most state medical boards have online complaint forms. The board’s response is usually slow, but the documentation persists, and patterns of complaint against a single provider do eventually surface in board action.
The trans plus medical-fatphobia compound issue
I want to spend the time this section deserves, because the trans plus-size patient navigating American healthcare is exposed to a compound of biases that no single section in any general article on healthcare access can fully address, and the assumption that the strategies above translate directly is wrong in important ways. I am writing this section as a cis woman who has done the listening work and consulted with trans collaborators on the specifics, but I would direct anyone who lives at this intersection to Dr. Sand Chang’s writing and to the trans-led healthcare collectives that have built more specific resources than I can offer in a paragraph.
The compound is this. A trans patient walks into a medical setting and may already be navigating misgendering, inappropriate questions about transition status that are unrelated to the visit, refusal of providers to use chosen names, gatekeeping around gender-affirming care, and the structural problem that many electronic medical record systems still do not gracefully accommodate any gender other than M or F. A plus-size trans patient walks into the same setting carrying all of that, plus the medical-fatphobia stack documented in the research section above. The two biases interact rather than add. A provider who is dismissive of trans patients is statistically more likely to also be dismissive of fat patients, because both biases come from the same authoritarian framing of bodies as needing to be brought into compliance with norms.
The practical strategies for trans plus-size patients include, in addition to the general scripts above, the use of trans-specific directories like the GLMA (Health Professionals Advancing LGBTQ+ Equality) provider directory, the OutCare Health directory, and the regional networks maintained by groups like the National Center for Transgender Equality. These directories overlap only partially with HAES directories, which means the work of finding a provider who is competent across both axes often requires cross-referencing multiple lists and accepting that the candidate pool is smaller. Telehealth, again, expands the pool meaningfully.
The exam-room scripts also need adaptation. The 4-sentence opener for a trans plus-size patient might add a fifth sentence on chosen name and pronouns, delivered as part of the same framing, so that the provider hears the full set of expectations at once rather than piecemeal. The BMI-pushback script remains the same, but the trans patient should be prepared for providers to attempt to gatekeep gender-affirming care behind weight loss requirements, which has been documented as a pattern in surgical practices in particular. The response to that gatekeeping is the same as the response to any other inappropriate use of weight as a barrier. You ask the provider to name the standard of care for a cis patient with the same presentation, and you ask them to apply it.
The compounding effect is also psychological. The exposure to layered dismissal is more depleting than the exposure to a single layer, and the avoidance behaviors documented in the Sutin research are correspondingly more pronounced. Trans plus-size patients I have spoken with describe going years without primary care because the prospect of running the full gauntlet for a routine annual is not worth the symptom-level risk. That is not a failure of self-care. It is a rational response to a hostile environment, and the solution is structural, which means the patient needs allies in the system who will do some of the navigation work for them. A trans-competent and HAES-aligned PCP is one of those allies. Finding one is a project. Worth it.
The 3-move checklist for this week
Reading this article and not doing anything with it is the most common outcome and I want to interrupt that. The work I am asking for this week is small. Three moves. None of them require a referral, an appointment, or money. All of them are things you can do from your phone in the next seven days. If you do these three things this week, you will be measurably closer to the doctor relationship you actually need than you were yesterday. Do not skip them.
Move one. Open a browser, search for “ASDAH HAES practitioner directory,” filter by your state, and download or screenshot the list of any providers in your zip code or within driving distance. If there are no providers in your state, do the same with the Plus Size Birth provider list and the Be Nourished directory. Add any names you find to a single document or note on your phone. Title the note “My Doctor List.” This list is the asset you are building. It is going to grow over time.
Move two. Open a new note and write the 4-sentence pre-visit opener for yourself, with your name, the symptom or screening you would bring to a first visit, and your specific hoped-for outcome. Memorize it. Practice saying it out loud in your car or in the shower until it sounds natural. The reason to do this when you are not in distress is so that you have it ready when you are.
Move three. Schedule the second-opinion appointment. If you have a current provider who has dismissed a symptom, fired you in spirit if not in writing, or made you dread the exam room, schedule a consultation with one of the new names on your list. It does not need to be a transfer of care yet. It is a consultation. You are gathering information. The appointment itself is the move. Booking it is the practice of believing that you are entitled to better care than you have been getting.
That is the assignment. Three moves. Within seven days. The list, the script, the appointment. You do not have to fix the entire American medical system this week. You have to do the three small things that put you in motion. The motion is the win. The Brookhaven exam room I started this article with is the floor. I built up from it by doing exactly these three things, in that order, in November of 2024. By the spring of 2025 I had a new PCP, a new OB-GYN, a referral to cardiology that produced an actual diagnosis for the palpitations (benign premature ventricular contractions, monitored, not weight-related), and a relationship with care that I no longer dread. That is what is on the other side of this. Go build the list.